
Beyond the Biopsy: A New Dimension in Understanding Liver Disease
For decades, the microscopic slide has been the primary window into the health of the human liver. Pathologists examine thin, two-dimensional slices of tissue to diagnose conditions ranging from fatty liver disease to cirrhosis, relying on visual cues to assess the extent of damage. But the liver isn’t flat; it’s a complex, three-dimensional organ whose intricate architecture is crucial to its function. A study published February 18, 2026, in Science Advances details a breakthrough in visualizing this complexity – a method for reconstructing human liver tissue in 3D at a cellular level – and it’s already reshaping how researchers approach liver disease. This isn’t simply about prettier pictures; it’s about recognizing that a flattened view inherently misses critical information about how the liver works and fails.
The research, spearheaded by Dr. Kelly Stevens at the University of Washington and funded by a consortium of NIH institutes including the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), addresses a fundamental limitation in liver research. Current models often rely on 2D cell cultures, which, while useful for certain experiments, fail to replicate the liver’s intricate lobular structure – the functional units comprised of central veins, blood vessels, bile ducts, and specialized cells. Understanding how this structure degrades during cirrhosis, a severe form of scarring, has been particularly challenging. The team’s new technique, dubbed the LiverMap pipeline, offers a solution by allowing scientists to visualize the spatial relationships between these components in a way previously impossible.
The LiverMap pipeline begins with tissue samples obtained from both healthy and cirrhotic livers – specifically, six patients undergoing tumor removal and three receiving liver transplants. Researchers employed fluorescent antibodies to label different cell types within the tissue, then used a chemical process to render the samples transparent. These clarified tissue sections were then imaged under a high-powered microscope, and sophisticated computer software assembled the resulting images into detailed 3D reconstructions. What they discovered wasn’t merely a confirmation of existing knowledge, but a revelation of previously unseen architectural disruptions. The team, including Wes Fabyan and Chelsea Fortin, found that cirrhosis doesn’t just involve scarring; it fundamentally rearranges the organization of cells and blood vessels across multiple lobules, disrupting the liver’s carefully orchestrated internal landscape.
Based on the original nih.gov report.
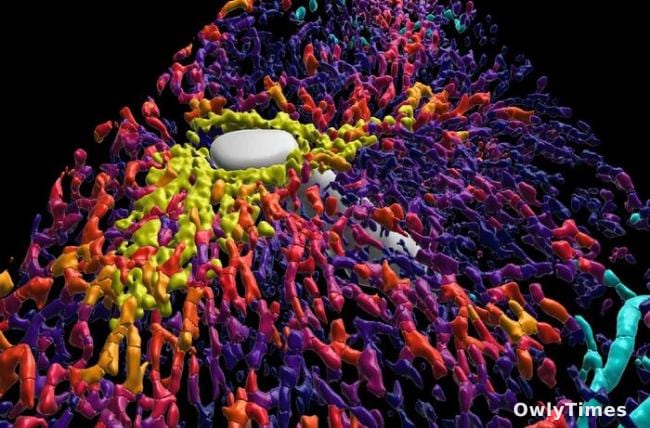
Specifically, the 3D reconstructions revealed a decrease in cells producing a key liver enzyme in cirrhotic tissue, alongside a reduction in the number of central veins. Perhaps most strikingly, the network of bile ducts – essential for digestion – became significantly fragmented. This fragmentation isn’t simply a consequence of scarring; it appears to be an active component of the disease process, suggesting that bile flow disruption may contribute to the progression of cirrhosis. This is a critical distinction. Headlines proclaiming “3D liver reconstruction reveals changes in cirrhosis” are accurate, but they often obscure the nuance: the study isn’t just showing changes, it’s revealing how those changes are spatially organized and interconnected, offering clues to the underlying mechanisms of the disease.
However, it’s important to acknowledge the limitations of this groundbreaking work. The LiverMap pipeline, while a significant advancement, doesn’t yet capture the full depth of a human liver lobule. The reconstructed volumes represent a substantial improvement over 2D imaging, but they are still partial representations of the organ’s complete architecture. Furthermore, the study utilized a relatively small sample size – nine patients in total. While the findings are compelling, larger, more diverse cohorts will be needed to validate these observations and determine the extent to which they generalize across different populations and stages of cirrhosis. The samples themselves, obtained from patients undergoing other procedures, also introduce potential biases.
Looking ahead, Dr. Stevens envisions a future where these 3D “organ maps” become the blueprints for bioprinting functional liver tissue for transplantation. “We don’t yet have the ‘blueprints’ of human organs to feed into bioprinters,” she explains. “If the maps aren’t right, the organs produced will not be functional.” This is an ambitious goal, but the LiverMap pipeline represents a crucial first step. The immediate next step for researchers will be refining the technique to achieve complete lobule reconstructions and tracking how these structural changes evolve as cirrhosis progresses. But perhaps the most pressing question now is: can these detailed 3D maps identify early structural changes that precede clinical symptoms, offering a window for preventative intervention before irreversible damage occurs? That’s the scenario clinicians and patients will be watching for closely in the coming years.





