
Beyond the Cavity Count: Why Regional Disparities in Children’s Oral Health Demand a Closer Look
The headline reads “15% of US Children Face Oral Health Problems,” and it’s a figure that understandably prompts concern. But focusing solely on that national average obscures a far more critical story: the stark and persistent geographic inequalities in children’s dental health. New data analysis from the Kaiser Family Foundation (KFF), released in 2024, reveals a landscape where a child’s zip code is a surprisingly strong predictor of their likelihood of experiencing toothaches, bleeding gums, or cavities. This isn’t simply a matter of access to dentists, though that’s a significant factor; it’s a complex interplay of socioeconomic conditions, preventative care, and public health infrastructure that demands a more nuanced understanding. The KFF analysis, built upon data from the U.S. Data Resource Center for Child & Adolescent Health, isn’t finding a problem—it’s quantifying a long-standing vulnerability that’s disproportionately affecting children in specific regions.
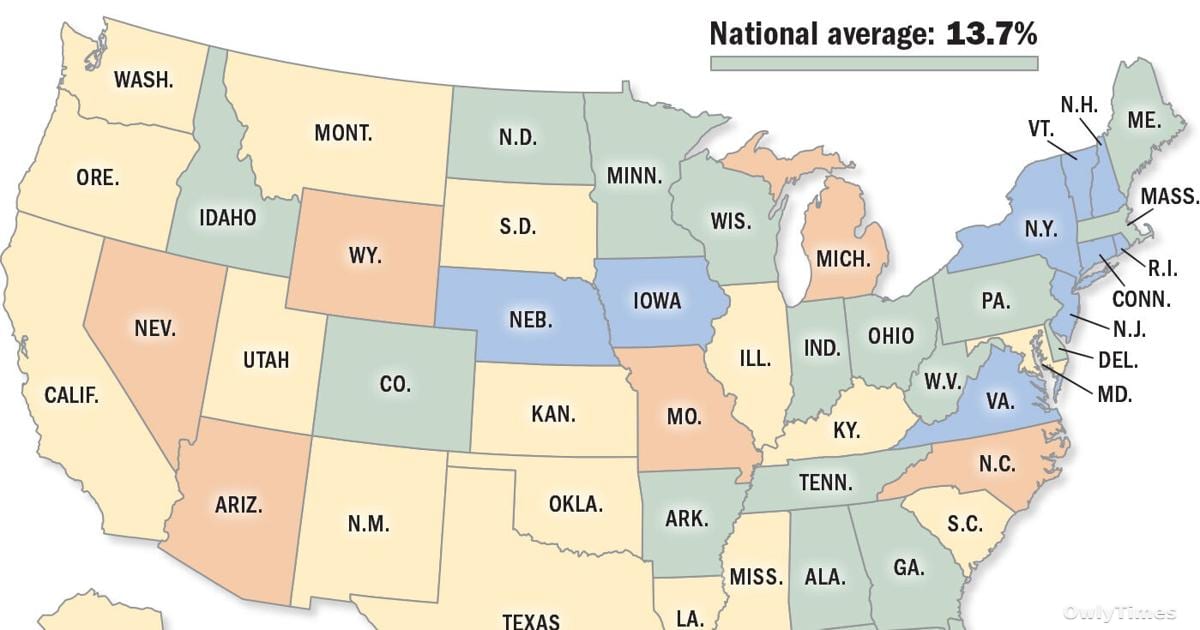
The KFF study assessed oral health by examining responses to three key questions: had the child experienced a toothache in the past year, reported bleeding gums, or been diagnosed with decayed teeth or cavities. This methodology, while relying on parental reporting, provides a standardized measure across states, allowing for meaningful comparison. What the data reveals is a significant range. While Virginia reports only 8.4% of children experiencing these issues, Wyoming leads the nation with a concerning 19%. Several states cluster in the middle, but the pattern is clear: the Mountain West and parts of the South consistently show higher rates of reported oral health problems. Louisiana, for example, registers at 16%, placing it as the seventh-highest state in the nation. This isn’t a trivial difference; a nearly 11 percentage point gap between the best and worst states translates to tens of thousands of children experiencing preventable pain and potential long-term health consequences.
Reporting from NOLA.com informs this analysis.
The Economic Roots of a Preventable Crisis
It’s tempting to attribute these disparities to individual behaviors – diet, brushing habits, and so on. However, a deeper dive into the demographics of these states reveals a strong correlation between childhood oral health and economic hardship. States with higher rates of poverty and limited access to employer-sponsored dental insurance consistently appear at the top of the KFF’s list. Nevada and North Carolina, both reporting 17.5% rates of childhood oral health problems, also have significant populations struggling with economic insecurity. This isn’t coincidental. Preventative dental care – regular check-ups, fluoride treatments, and sealants – are often the first casualties of tight household budgets. When families are forced to choose between groceries and a dentist appointment, dental health often loses out. Moreover, states with robust public health programs, like those offering school-based dental screenings and low-cost care, tend to have lower rates of reported problems, suggesting that targeted interventions can make a difference.
What the Data Doesn’t Tell Us: Nuances and Missing Pieces
While the KFF data provides a valuable snapshot, it’s crucial to acknowledge its limitations. The reliance on parental reporting introduces potential for recall bias – parents may not accurately remember or report on their child’s dental experiences. Furthermore, the data doesn’t differentiate between the severity of oral health problems. A minor toothache is not equivalent to extensive decay requiring significant intervention, yet both are counted equally in these statistics. Perhaps most importantly, the data doesn’t illuminate the reasons behind the disparities. Is it solely economic, or are there cultural factors, geographic barriers to care (rural areas with limited dental practices), or variations in water fluoridation policies at play? The KFF analysis establishes where the problems are, but further research is needed to understand why they exist in these specific locations.
Beyond Treatment: The Future of Pediatric Oral Health Research
The next critical step isn’t simply expanding dental access, though that remains vital. It’s understanding the root causes of these regional disparities and tailoring interventions accordingly. Researchers need to investigate the interplay between socioeconomic factors, public health policies, and individual behaviors in these high-risk states. Specifically, studies should focus on the effectiveness of school-based dental programs, the impact of Medicaid expansion on children’s oral health, and the role of community health workers in promoting preventative care. We also need to move beyond simply counting cavities and start tracking the long-term consequences of untreated dental disease – its impact on school performance, nutrition, and overall quality of life. As policymakers debate funding for public health initiatives, will they prioritize preventative care for children, particularly in the states where it’s needed most? The answer to that question will determine whether the 15% figure remains a persistent national shame, or begins to decline.





