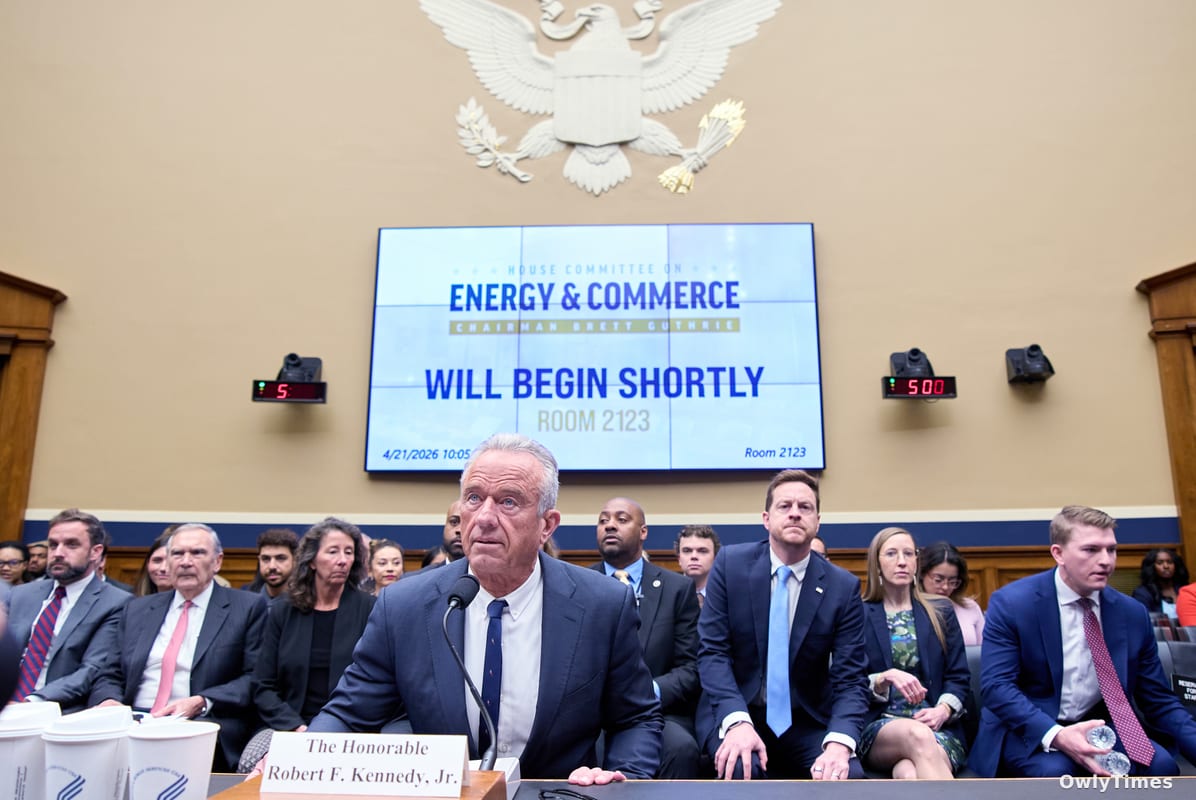

The recent series of congressional hearings featuring Health Secretary Robert F. Kennedy Jr. serves as a critical stress test for the intersection of public health policy and political loyalty. While the public discourse often centers on the theater of partisan clashes, the scientific question at hand is whether the Department of Health and Human Services (HHS) can maintain the integrity of evidence-based medical guidance while navigating a mandate increasingly driven by political, rather than clinical, priorities. Kennedy’s testimony this week before the U.S. Senate Finance Committee and the Senate Committee on Health, Education, Labor and Pensions (HELP) highlighted a widening chasm between the administration’s stated "historic wins"—such as nutrition education and the Rural Health Transformation Fund—and the growing alarm among lawmakers regarding the erosion of trust in national immunization programs.
It is vital to distinguish between the agency’s self-reported successes and the reality of its operational landscape. Headlines frequently focus on Kennedy’s contentious exchanges with Democrats, yet the deeper scientific concern lies in his unilateral modifications to the childhood vaccine schedule. These changes were enacted without the consultation of external advisors, a move that deviates from the established procedural rigor designed to insulate health policy from ideological shifts. Kennedy’s defense, particularly his assertion that the measles vaccine prevents infection in 97% of recipients, aligns with established immunological data. However, this scientific affirmation stands in stark contrast to the climate of vaccine skepticism that has permeated his tenure, a tension made tangible by the 2025 surge in measles cases, which reached levels unseen in the United States for three decades.
Limitations to consider include the disconnect between the administration's "TrumpRx" discount platform and market realities. When Senator Elizabeth Warren challenged the program by comparing the $200 cost of Protonix on the site to the $16 price available at retail chains like Costco, Kennedy cited the distinction between brand-name and generic pricing. This suggests a potential structural inefficiency in how the department navigates pharmaceutical markets, leaving patients to bear the burden of these discrepancies. Furthermore, the political precariousness of Kennedy’s position cannot be ignored. With President Trump having recently dismissed high-profile cabinet members like Kristi Noem, Pam Bondi, and Lori Chavez-DeRemer, Kennedy’s ability to influence long-term policy is increasingly tied to his standing within a rapidly shifting executive branch.
The legislative tension is perhaps best exemplified by Senator Bill Cassidy, who provided the tie-breaking vote for Kennedy’s confirmation last February. Despite having initially secured a commitment from Kennedy to collaborate on hiring and adhere to existing vaccine policies, Cassidy’s recent questioning signals a cooling of that relationship. While Cassidy maintains a focus on broader issues like Medicare Advantage, his pointed inquiry regarding whether the next director of the Centers for Disease Control and Prevention will have the autonomy to act independently of political appointees suggests a growing institutional anxiety. This concern is likely compounded by the recent departure of former CDC director Susan Monarez, who was ousted following policy disagreements with Kennedy.
Moving forward, the focus must shift from political rhetoric to measurable health outcomes. The next reading of national immunization data will serve as a definitive metric for the efficacy of the department’s current messaging strategies. Additionally, the administration’s ability to reconcile its stated goals—such as reducing exposure to glyphosate—with the President’s executive orders favoring increased production of such chemicals remains a critical contradiction to monitor. The success of the agency’s mission to foster a healthier nation will ultimately be judged not by promotional videos or legislative testimony, but by the stabilization of public health indicators that have seen significant volatility over the past 15 months.