
The narrative surrounding the opioid crisis has often focused on escalating numbers, a seemingly relentless climb in overdose deaths. But a recent analysis of data through 2024 reveals a significant, and cautiously optimistic, shift: opioid overdose deaths are falling. While headlines proclaim a turning point, a closer examination of the data – and the complex interplay of policy changes and evolving drug supplies – reveals a more nuanced picture. The decline, while substantial, doesn’t erase the devastating gains the crisis made during the pandemic, and emerging federal policy shifts threaten to stall or even reverse this progress. Understanding how these numbers are changing, and for whom, is crucial to building a sustainable response.
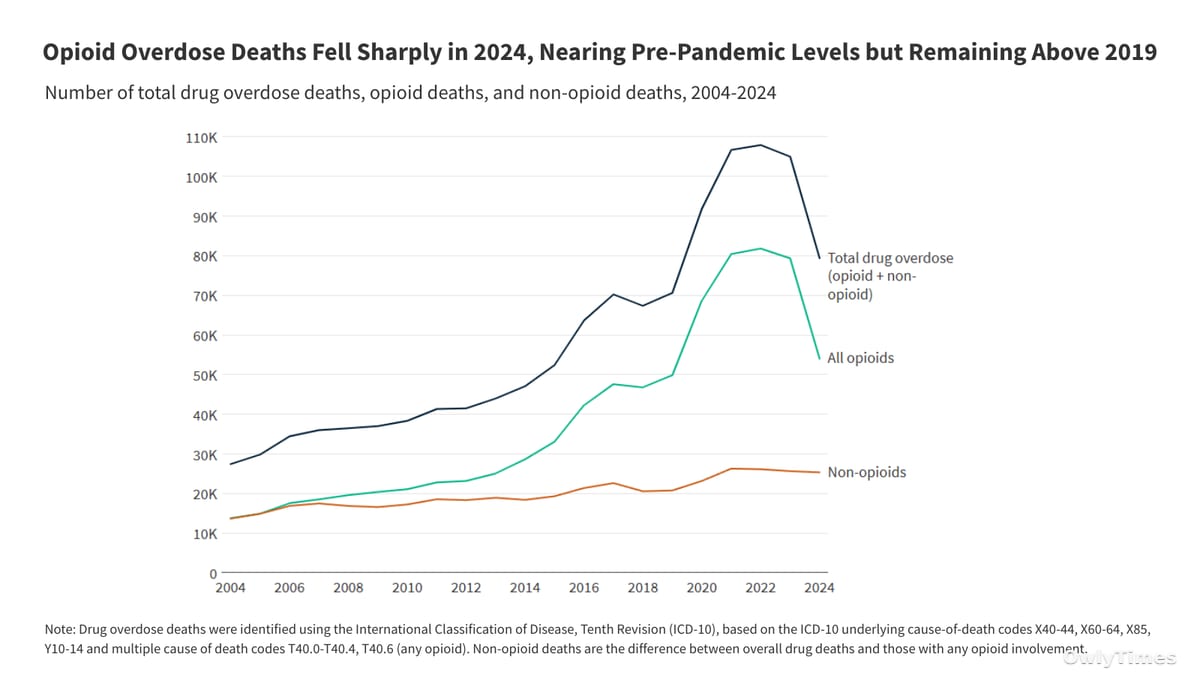
Since 2017, when the opioid epidemic was officially declared a public health emergency by the Department of Health and Human Services, over half a million lives have been lost. Initially fueled by prescription opioids and heroin, the crisis has become overwhelmingly dominated by illicit synthetic fentanyl, a substance exponentially more potent than morphine. By 2023, the Drug Enforcement Administration (DEA) reported that the majority of counterfeit opioid pills contained a potentially lethal dose of fentanyl. The impact is widespread; a 2022 survey by the Kaiser Family Foundation (KFF) found that nearly one in three adults (29%) reported either personal addiction or a family member’s struggle with opioids. The recent decline in deaths – from 79,358 in 2023 to 54,045 in 2024 – represents a 32% decrease, a statistically significant drop that demands attention. However, it’s vital to remember that even with this improvement, the current death toll remains above pre-pandemic levels, approximately 4,200 higher than in 2019.
Original reporting: kff.org.
The reasons behind this decline are likely multifaceted. The analysis points to a combination of policy interventions, including expanded access to treatment and the life-saving drug naloxone, increased public awareness campaigns regarding the dangers of counterfeit pills, and supply-side efforts to disrupt the flow of fentanyl and its precursor chemicals. Notably, DEA testing indicated a potential decrease in the potency of fentanyl found in counterfeit pills, suggesting a shift in the illicit supply. These factors likely worked in concert, but attributing specific weight to each remains a challenge. It’s also important to note that provisional data from the Centers for Disease Control and Prevention (CDC) suggests this downward trend has continued into 2025, though these numbers are still subject to revision.
However, the positive trend is shadowed by a series of recent federal policy changes that could jeopardize future progress. Budget cuts, staffing reductions within key agencies, and reductions in federal grants supporting state and local programs all threaten to undermine the infrastructure built to combat the crisis. Perhaps most concerning is the shift towards a more enforcement-focused approach, exemplified by the designation of illicit fentanyl as a “Weapon of Mass Destruction.” While intended to signal the severity of the threat, this designation could divert resources from crucial public health initiatives like harm reduction and treatment. The tension here is clear: a move away from evidence-based, compassionate care towards punitive measures risks exacerbating the problem, particularly for vulnerable populations.
Examining demographic variations reveals stark disparities. In 2024, opioid death rates were highest among adults aged 26-64, American Indian/Alaska Native (AIAN) individuals, Black individuals, and males. While all groups experienced declines in death rates from 2023 to 2024, the rates remain significantly elevated compared to 2019, particularly for AIAN individuals (a 101% increase) and older adults (a 63% increase). This suggests that existing interventions may not be reaching these populations effectively, or that unique challenges within these communities require tailored solutions. The fact that rates among White individuals declined more substantially than other groups (-9%) may reflect greater access to opioid use disorder treatment, highlighting existing inequities in healthcare access.
Geographic variations are equally pronounced. In 2024, opioid death rates ranged from a low of 3.3 per 100,000 in Nebraska to a high of 38.6 per 100,000 in West Virginia. While all states saw declines, the magnitude of those declines varied considerably. West Virginia, despite experiencing one of the largest percentage decreases (-46%), still maintains the highest death rate nationally. This underscores the importance of localized strategies, recognizing that the drivers of the opioid crisis – and the effectiveness of different interventions – can vary significantly from state to state. The fact that roughly half of states remain above 2019 levels suggests that the pandemic’s impact continues to reverberate, and that the timing of fentanyl’s spread across the country has created uneven recovery trajectories.
Looking ahead, the critical question isn’t simply whether overdose deaths will continue to fall, but for whom and at what cost. Will the recent declines be sustained in the face of federal policy shifts? Will targeted interventions be developed to address the disparities observed among different demographic groups? And, crucially, will states continue to prioritize evidence-based public health approaches over punitive measures? The coming months and years will reveal whether the current downward trend represents a genuine turning point in the opioid crisis, or merely a temporary reprieve. We should be watching closely for changes in state-level policy regarding harm reduction services, particularly naloxone access, and monitoring whether the designation of fentanyl as a “Weapon of Mass Destruction” leads to increased arrests and incarceration rates, potentially driving opioid use further underground.





