
The resurgence of measles, a disease once considered functionally eradicated in the United States, isn’t simply a public health concern—it’s a stark indicator of eroding community immunity and the complex interplay between travel, vaccine hesitancy, and the logistical challenges of maintaining high vaccination rates. Recent confirmed cases in Illinois, specifically exposures at O’Hare International Airport and retail locations in Niles and Mount Prospect, demand a closer look not just at individual exposure risks, but at the systemic vulnerabilities that allow this highly contagious virus to regain a foothold. While headlines focus on potential exposure locations, the underlying story is about the delicate balance required to protect populations from preventable diseases, and how easily that balance can be disrupted.
Navigating Exposure Risks in Cook County
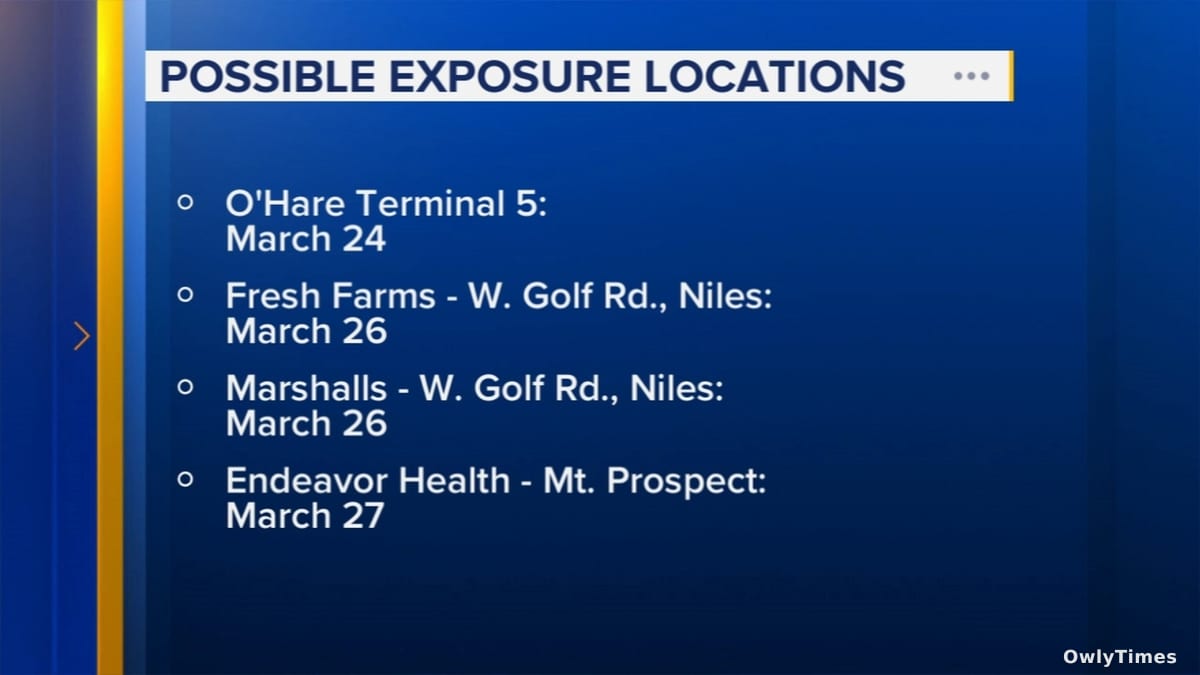
On Wednesday, April 1, 2026, the Cook County Health department announced a confirmed case of measles in an individual who visited several public locations the previous week. Specifically, exposure risks were identified at Terminal Five of O’Hare International Airport last Tuesday between 10:45 a.m. and 2:30 p.m., as well as at the Marshalls and Fresh Farms stores on Golf Road in Niles last Thursday, and an immediate care center in Mount Prospect on Friday. These locations represent a diverse range of potential exposures – a major transportation hub connecting individuals from across the globe, everyday retail environments, and a healthcare setting where individuals may already be immunocompromised. The significance of the airport exposure cannot be overstated; measles is highly contagious, and air travel facilitates rapid dissemination across geographic boundaries. It’s crucial to understand that an infected individual is contagious four days before and four days after the appearance of the rash, meaning exposures could have occurred before the individual even knew they were infected.
Drawn from abc7chicago.com.
Beyond Individual Cases: Assessing Community Immunity
The immediate response to these exposures – advising individuals to monitor for symptoms like rash, high fever, cough, runny nose, and red, watery eyes – is vital, but it addresses the consequence, not the cause. The core issue is declining immunity within communities. Measles has a very high R0 value – the average number of secondary infections caused by a single infected individual in a completely susceptible population – estimated between 12 and 18. This means it’s far more contagious than influenza (R0 of 1.2-3) or even COVID-19 (original strain R0 of 2-3). Achieving herd immunity requires a vaccination rate of approximately 95%. While national vaccination rates for measles, mumps, and rubella (MMR) vaccine remain relatively high, at around 93% according to the Centers for Disease Control and Prevention data from late 2025, this figure masks significant regional variations and pockets of unvaccinated individuals. These pockets, often linked to philosophical or religious objections to vaccination, or logistical barriers to access, are where outbreaks are most likely to originate and spread. The current situation in Cook County serves as a potent reminder that a 93% national average doesn’t guarantee protection for everyone.
The Role of Travel and Delayed Diagnosis
The O’Hare exposure highlights the role of international travel in reintroducing measles to the U.S. While the source of this particular infection hasn’t been publicly identified, a significant proportion of U.S. measles cases in recent years have been linked to travelers returning from countries experiencing outbreaks, such as those in Europe, Asia, and Africa. This isn’t a new phenomenon, but the increasing volume of international travel post-pandemic amplifies the risk. Furthermore, a delay in diagnosis can exacerbate the spread. Measles symptoms are initially non-specific, resembling common viral illnesses. This can lead to individuals unknowingly spreading the virus before a definitive diagnosis is made, as potentially occurred in this case. The fact that the individual sought care at an immediate care center, rather than a primary care physician with a potentially more comprehensive vaccination history, may have contributed to this delay.
Limitations to Consider and Future Research
It’s important to acknowledge the limitations of the available information. The current reporting focuses on identified exposure locations, but doesn’t provide details about the infected individual’s vaccination status, travel history, or the genetic sequencing of the virus – information that would be crucial for understanding the outbreak’s origin and potential spread. Public health officials are understandably cautious about releasing personal medical information, but greater transparency regarding viral strain identification could help track the outbreak’s evolution. Additionally, the reporting doesn’t address the capacity of local healthcare systems to respond to a potential surge in cases, or the availability of MMR vaccine in the affected areas.
Looking ahead, research needs to focus on understanding the factors driving vaccine hesitancy and developing targeted interventions to address misinformation. Furthermore, investment in robust surveillance systems is critical for early detection and rapid response to outbreaks. We need to move beyond simply tracking cases and begin actively monitoring community immunity levels at a granular level – down to the zip code, or even the school district. The question isn’t if another measles outbreak will occur, but when, and whether we will be adequately prepared to contain it. Specifically, public health officials should be prepared to answer: how will vaccination campaigns be rapidly deployed to areas experiencing localized outbreaks, and how will access to vaccination be ensured for vulnerable populations? The answer to these questions will determine whether measles remains a rare, preventable disease, or a recurring threat to public health.





