
The promise of rural healthcare often hinges on infusions of federal funding, but the actual impact of those dollars is rarely straightforward. Missouri is poised to receive over $216 million through a new federal initiative designed to modernize care in rural communities – a substantial sum, yet one arriving with a complex set of conditions and existing challenges. While headlines tout a lifeline for struggling hospitals and clinics, a closer look reveals a process still unfolding, dependent on state legislative action, and built upon a foundation of existing systemic vulnerabilities. This isn’t simply about adding money to the system; it’s about whether this funding can overcome deeply entrenched barriers to access and quality of care in Missouri’s most underserved regions.
The award, granted on December 29th, stems from a sweeping federal rural health initiative spearheaded by the Centers for Medicare & Medicaid Services (CMS). However, the initial announcement wasn’t a green light for immediate spending. CMS required a revised budget from Missouri, a request submitted and awaiting final approval by the end of February. This initial hurdle underscores a common tension in federal grant programs: the need for detailed planning and justification, which can delay the actual deployment of funds. Even with CMS approval, the money isn’t yet accessible. It requires a subsequent appropriation from the Missouri legislature, introducing a political layer that could alter the intended scope or timeline of the projects. This two-step process – federal approval followed by state appropriation – means the true impact of the $216 million won’t be known for several months.
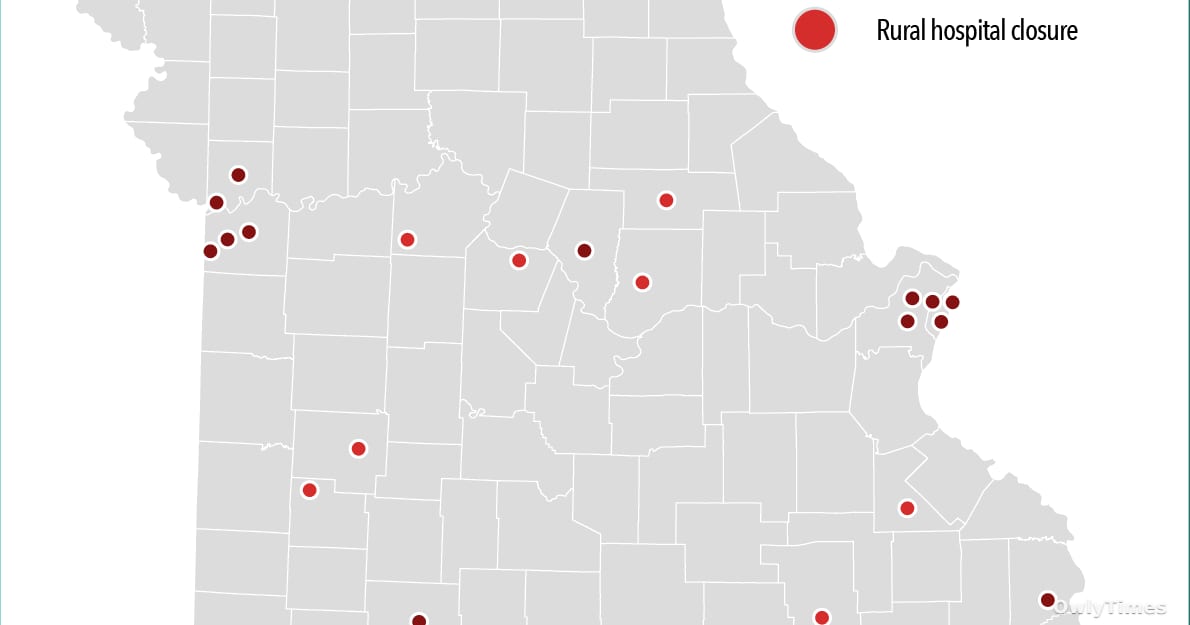
Based on the original columbiamissourian.com report.
The core of the initiative, as described by CMS, focuses on addressing structural barriers to healthcare delivery. These aren’t simply about a lack of doctors; they encompass issues like outdated infrastructure, limited access to broadband internet (critical for telehealth), workforce shortages extending beyond physicians to include nurses and technicians, and the financial instability of rural hospitals. The funds are intended to support a range of projects, from upgrading electronic health records to expanding telehealth services and bolstering the rural healthcare workforce. Dr. Jeanne Abbott, Managing Editor for Print at the Columbia Missourian, notes that the initiative’s success will depend on a holistic approach, stating, “Rural hospitals need more than just money; they need strategic investments in technology, workforce development, and innovative care models.” The emphasis on infrastructure is particularly noteworthy, as many rural facilities operate with aging equipment and limited capacity.
However, the scale of the problem demands careful consideration. While $216 million is a significant investment, it must be viewed in context. Missouri has 139 rural hospitals, many of which are operating on razor-thin margins. According to the Missouri Hospital Association, nearly half of rural hospitals in the state are operating at a loss. Dividing the $216 million across all these facilities yields an average of roughly $1.55 million per hospital – a substantial amount, but potentially insufficient to address all their needs. Furthermore, the funds are likely to be distributed based on a competitive application process, meaning not all hospitals will receive equal shares. This raises concerns about equitable distribution and the potential for exacerbating existing disparities. Brittany Hilderbrand, Higher Education and Health Editor at the Columbia Missourian, points out that “the competitive nature of the grant process could inadvertently favor larger, better-resourced rural hospitals, leaving smaller, more vulnerable facilities behind.”
Limitations to consider include the inherent challenges of implementing large-scale projects in rural areas. Workforce recruitment and retention remain significant obstacles. Attracting healthcare professionals to rural communities often requires offering competitive salaries and benefits, as well as addressing quality-of-life concerns like access to education and cultural amenities. The initiative’s success will hinge on addressing these factors, not just providing funding for new programs. Additionally, the long-term sustainability of these projects is uncertain. Without a sustained commitment to rural healthcare funding, the gains made through this initiative could be eroded over time. The reliance on legislative appropriation also introduces a degree of political risk, as future budget decisions could impact the availability of funds.
Looking ahead, the next crucial step is the Missouri legislature’s decision on appropriation. The debate will likely center on how best to allocate the funds to maximize their impact. Will the focus be on shoring up existing hospitals, expanding telehealth services, or investing in workforce development? The answer will have profound implications for the future of rural healthcare in Missouri. Beyond that, researchers will need to rigorously evaluate the effectiveness of the funded projects. Tracking key metrics like hospital closure rates, access to care, and health outcomes will be essential to determine whether the initiative is achieving its intended goals. A critical question remains: will this infusion of funding truly transform rural healthcare in Missouri, or will it simply provide a temporary reprieve from a deeper, systemic crisis? The coming months will be pivotal in determining the answer.





