
The quiet revolution in maternity care isn’t happening with flashy new procedures, but with a shift in how data is used. The recent $2.75 million investment by NYC Health + Hospitals in PeriGen’s PeriWatch Vigilance technology isn’t simply about adding another tool to the labor and delivery ward; it’s a response to a persistent, and often overlooked, problem: the sheer volume of information clinicians must process during a high-stakes event like childbirth. While headlines tout a potential 12% reduction in unexpected complications – a figure derived from a single U.S. healthcare system’s experience with the technology – the real story lies in understanding how this system aims to improve outcomes, and what limitations remain in relying on algorithms to augment human judgment.
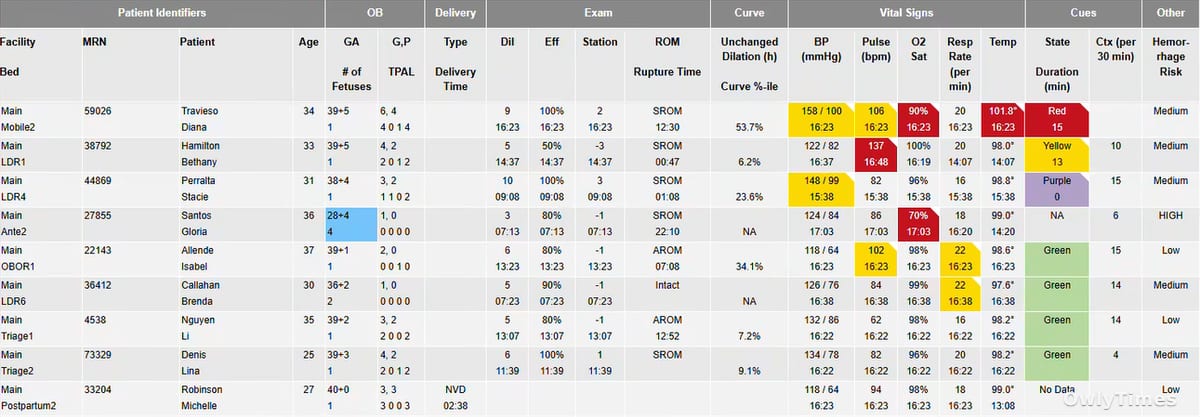
The core of PeriWatch Vigilance is its “Vigilance Hub Board,” a centralized display consolidating vital signs, fetal monitoring data, and labor progression information for each patient. This isn’t new data; hospitals have collected this information for decades. What is new is the system’s ability to present a 4- or 12-hour trend of this data, color-coded to flag potential issues requiring immediate attention. This addresses a critical challenge in obstetrics: the cognitive load on clinicians, particularly during busy shifts. A nurse or physician monitoring multiple patients simultaneously can easily miss subtle but significant changes in a patient’s condition. The system, as Matthew Sappern, CEO of PeriGen, notes, aims to bring “more consistent, data-driven care to the bedside.” This consistency is particularly crucial within a large, diverse system like NYC Health + Hospitals, which delivers approximately 15,000 babies annually across its 11 hospitals.
Original reporting: nychealthandhospitals.org.
The emphasis on “equity” in the rollout, highlighted by NYC Health + Hospitals Chief Women’s Health Officer Wendy Wilcox, MD, MPH, MBA, FACOG, is also a key aspect of this investment. Wilcox specifically mentioned the goal of closing equity gaps for Black and Brown women, who experience disproportionately higher rates of maternal morbidity and mortality. The promise here isn’t simply better monitoring, but a standardization of care that could mitigate implicit biases and ensure all patients receive the same level of vigilance. However, it’s vital to acknowledge that technology alone cannot solve systemic inequities. Data algorithms are trained on existing datasets, and if those datasets reflect existing biases – for example, if certain populations are historically under-monitored or misdiagnosed – the algorithm may perpetuate those biases.
The 12% reduction in unexpected complications reported by one U.S. healthcare system is encouraging, but it’s crucial to understand the context. This figure represents a relative risk reduction, meaning a 12% decrease compared to the baseline complication rate before implementing the system. The absolute risk reduction – the actual number of complications prevented – would be a more informative metric, and one that NYC Health + Hospitals will need to track closely as it expands the program. Furthermore, the study’s methodology and the specific patient population involved aren’t detailed in the press release, making it difficult to assess the generalizability of these findings. It’s also important to note that “unexpected complications” is a broad category, encompassing a wide range of events with varying degrees of severity.
Limitations to Consider
Despite the potential benefits, relying on automated systems introduces inherent limitations. Over-reliance on alerts could lead to “alarm fatigue,” where clinicians become desensitized to warnings and miss genuine emergencies. The system is designed to augment clinical judgment, not replace it. Furthermore, the effectiveness of PeriWatch Vigilance depends on accurate data input and proper system maintenance. A malfunctioning sensor or a data entry error could generate false alarms or mask critical information. The system’s utility also extends only as far as the data it receives; it cannot account for factors outside of physiological measurements, such as a patient’s social determinants of health or their emotional state.
Beyond the Hub Board: Expanding the Scope of Vigilance
The initial rollout at NYC Health + Hospitals/North Central Bronx is just the first step. The system will be deployed across all 11 hospitals later this year, requiring extensive training for staff and ongoing monitoring of its performance. The true impact of this investment won’t be fully realized for several years, as the system collects data and allows for refinement of algorithms and clinical protocols. A key next step will be integrating PeriWatch Vigilance with other electronic health record (EHR) systems, creating a more seamless flow of information and reducing the risk of data silos.
What Happens When the Algorithm Disagrees?
Looking ahead, the most critical research question isn’t whether the system can identify risk, but how clinicians will respond when the system’s assessment conflicts with their own. Will they defer to the algorithm, even when their clinical intuition suggests otherwise? Or will they use the system as a second opinion, carefully weighing the data alongside their own expertise? The answer to this question will determine whether PeriWatch Vigilance truly enhances patient safety, or simply adds another layer of complexity to an already challenging field. As NYC Health + Hospitals begins to gather its own data, clinicians and researchers should be prepared to address this tension head-on, and to develop clear guidelines for navigating these inevitable disagreements.









