
Beyond the Headlines: Understanding the Current Measles Exposure in Colorado
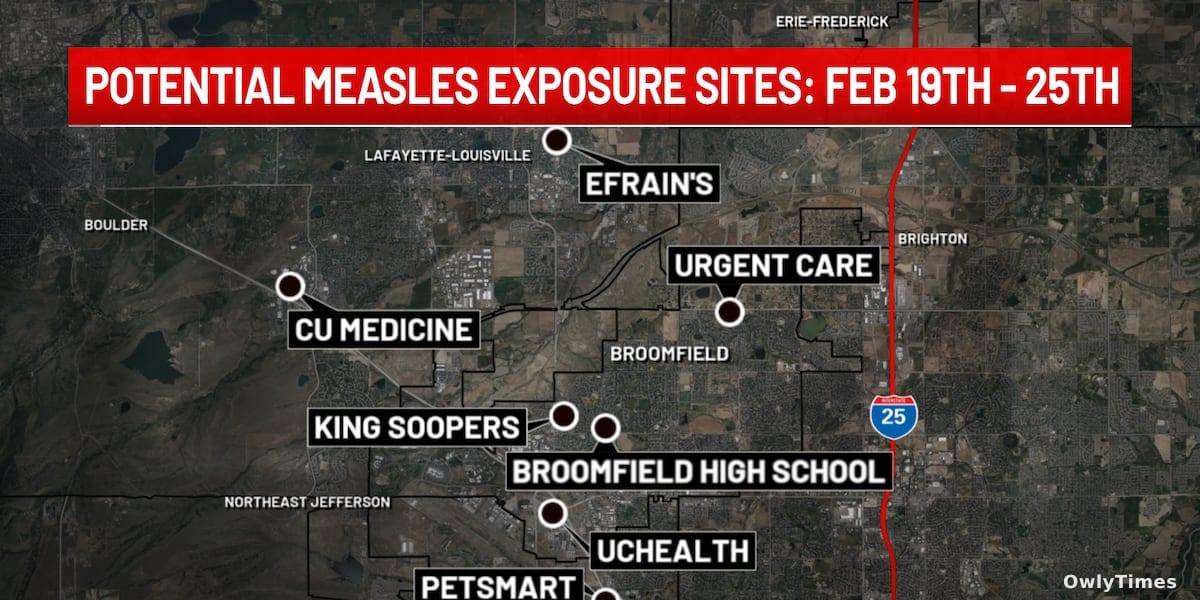
The recent confirmation of a measles case in Broomfield County, Colorado, isn’t simply a return of a disease declared eliminated in 2000; it’s a stark reminder of the ongoing vulnerability created by declining vaccination rates and the complex interplay between individual choices and public health. While initial reports from KKTV and the Colorado Department of Public Health and Environment (CDPHE) focus on potential exposure locations – Broomfield High School, King Soopers, Petsmart Walnut Creek, Efrains Mexican Restaurant, Advanced Urgent Care, UCHealth Broomfield Hospital Emergency Department, and CU Medicine Family Medicine Clinic – the significance lies in what this single case reveals about the fragility of our collective immunity. The CDPHE is urging anyone who visited these locations between February 19th and February 25th to monitor for symptoms, which can develop up to 21 days after exposure. This isn’t about fear-mongering, but a calculated response based on the highly contagious nature of the measles virus.
Source material: kktv.com.
The core issue isn’t the virus itself, but its ability to exploit gaps in immunity. Measles has a reproduction number (R0) of 12-18, meaning each infected person, on average, will infect 12 to 18 others in a completely susceptible population. This is significantly higher than influenza (R0 of 1.2-3) or even COVID-19 (varying strains, but generally 2-5). The case in Broomfield County involves an unvaccinated child, a detail the CDPHE explicitly stated. While vaccination status is a personal decision, measles is a disease where individual protection directly impacts community safety. Prior to the widespread measles, mumps, and rubella (MMR) vaccine, nearly all children contracted measles. Now, the virus persists primarily in pockets of unvaccinated individuals, creating opportunities for outbreaks like this one. The CDPHE’s response – identifying exposure locations and advising symptom monitoring – is a containment strategy, attempting to limit secondary spread from this initial case.
Mapping the Exposure Window and Symptom Awareness
The CDPHE’s public health advisory details a specific timeframe for potential exposure at each location. For example, individuals who visited Broomfield High School on February 19th, 20th, or 23rd could develop symptoms as late as March 16th. This 21-day window is crucial because it accounts for the measles incubation period – the time between infection and the onset of symptoms. Symptoms themselves are non-specific initially, often beginning with a fever, cough, runny nose, and red eyes. The characteristic rash, which starts on the face and spreads downwards, typically appears several days after the initial symptoms. This initial phase can mimic other common viral illnesses, making early diagnosis challenging. The CDPHE is urging anyone experiencing these symptoms, particularly if they visited one of the listed locations during the specified dates, to contact their healthcare provider before seeking care, to allow for appropriate precautions to be taken and prevent further spread within healthcare settings.
It’s important to note that the CDPHE isn’t simply listing locations; they are actively conducting contact tracing to identify and notify individuals who may have been directly exposed. This is a resource-intensive process, requiring trained public health professionals to interview the infected individual and map their movements. The fact that multiple locations are involved suggests a period of potential community spread before the case was identified and isolated. This highlights the importance of rapid diagnosis and reporting, as well as maintaining high vaccination coverage to minimize the impact of any future outbreaks. The advisory also underscores the potential for exposure in everyday settings – grocery stores, restaurants, schools – demonstrating that measles isn’t confined to specific populations or geographic areas.
Limitations to Consider: Data and Broader Trends
While the CDPHE’s response is appropriate, several limitations should be considered. The advisory relies on accurate recall of locations and times by the infected individual and those potentially exposed. Memory is fallible, and individuals may not accurately remember every detail of their movements. Furthermore, the advisory focuses on identified exposure locations. It’s possible the individual visited other places not currently listed, creating additional, unknown exposure risks. Nationally, the Centers for Disease Control and Prevention (CDC) reported 58 cases of measles in the US in 2024 as of February 29th, a significant increase compared to the 2023 total of 41 cases. This national trend is concerning, and Colorado’s case is part of a larger pattern of increasing measles incidence.
The decline in MMR vaccination rates is a key driver of this resurgence. Nationally, MMR coverage among kindergarteners is around 93%, but this figure masks significant variation at the state and local levels. Areas with lower vaccination rates are particularly vulnerable to outbreaks. It’s also crucial to acknowledge that vaccine hesitancy isn’t a monolithic phenomenon. It stems from a complex interplay of factors, including misinformation, distrust of medical institutions, and concerns about vaccine safety. Addressing these concerns requires nuanced communication and targeted outreach efforts, rather than simply dismissing vaccine hesitancy as irrational.
What Comes Next: Surveillance and Strengthening Immunity
The immediate next steps involve continued contact tracing by the CDPHE, monitoring for new cases, and encouraging vaccination. However, this incident should prompt a broader discussion about strengthening public health infrastructure and addressing the root causes of declining vaccination rates. The CDPHE should analyze the vaccination status of individuals affected by this outbreak to identify potential gaps in coverage and tailor interventions accordingly. Furthermore, increased investment in public health education and outreach is essential to combat misinformation and promote vaccine confidence.
Looking ahead, we should be asking: what proactive measures can be implemented to prevent similar outbreaks in the future? Will this case spur increased vaccination rates in Broomfield County and surrounding areas? And, critically, how can public health officials effectively communicate the risks and benefits of vaccination in a way that resonates with diverse communities? The answer to these questions will determine whether this measles case is an isolated incident or a harbinger of a larger resurgence of vaccine-preventable diseases.